Indice del volumen
Volume index
Comité Editorial
Editorial Board
Comité Científico
Scientific Committee
RENOVASCULAR HYPERTENSION DUE TO RENAL ARTERY STENOSIS IN KLIPPEL-FEIL SYNDROME
Ibańez-Valdés LdeF. MD, Foyaca-Sibat H. MD.
Department of Family Medicine, and Department of Neurology. University of Transkei. Umtata. South Africa.
lourdesdefatima@yahoo.comRev Electron Biomed / Electron J Biomed 2003;1(2):95-100.
- Nally JV, Barton DP. Contemporary approach to diagnosis and evaluation of renovascular hypertension. Urol Clin North Amer 2001;28(4):781-791.
- Koyanagi T, Nonomura K, Takeuchi I, Watari Y, Seki T, Kakizaki H. Surgery for renovascular diseases: a single-center experience in renovascularizing renal artery stenosis and aneurysm. Urol Int 2002;68(1):24-31.
- Clarke RA, Well D, Yip M. KFs Class Klippel-Feil syndrome. Amer J Hum Genet 1995:57(6):1364-1370.
- Hasan I, Wapnick S, Kutscher L, Couldwell T. Vertebral arterial dissection associated with Klippel-Feil syndrome in a child. Childs Nerv Syst 2002; 18(1):67-70.
- Patzer L, Basches S, Misselwitz J. Renal artery stenosis and aneurysmatic dilatation of arteria carotis interna in tuberous sclerosis complex. Pediatr Nephrol 2002;17(3):1193-196.
- Thomsen M, Krober M, Scheider U, Carsten C. Congenital limb deficiencies associated with Klippel-Feil syndrome. Act Orthop Scan 2000; 71(5):461-465.
- Fragoso R, Cid-Garcia A, Hernandez A, Nazara Z, Cantu JM. Frontonasal dysplasia in the Klippel-Feil syndrome: a new associated malformation. Clin Genet 1982;22:170-273.
- Clarke RA, Davis PJ, Tonkin J. Klippel-Feil syndrome associated with malformed larynx; case report. Ann Otol Rhinol Laryng 1994;103:201-207.
- McGaughran JM, Kuna P, Das V. Audiological abnormalities in the Klippel-Feil syndrome. Arch Dis Child 1998;79:352-355.
- Curcione DO, Mackenzie W. Klippel-Feil syndrome. Available online: http://www.gait.udel.edu/res695/homepage/pd_ortho/educate/clincase/klipfeil.htm
- Ogden CW,Jackson JE. The Klippel-Treanunay syndrome associated with renal artery aneurysm. Br. J. Urol 1993;71(5)617-618.
- Larson AR, Josephson KD, Pauli RM, Optiz JM, Williams MS. Klippel-Feil anomaly with Sprengel anomaly, omovertebral bone, thumb abnormalities, and flexion-crease changes: novel association or syndrome? Am J Med Genet 2001;101(2):158-162.
- Misra UK, Kalita J, Kapoor R. Postural hypotension in a patient with cervical myelopathy due to craniocervical anomaly. Cli Auton Res 1997 ;7(5):223-226.
- Steyn K, Thomas AG, Bradshaw , Laubscher R and Fourier J. Hypertension in South Africa adults: results from the Demographic and Health Survey, 1998. Journal of Hypertension 2001;19:1717-1725.
- Spence JD. Treatment options for renovascular hypertension. Expert Opin Pharmacother 2002;3(4):411-416.
- Nally JV, Barton DP. Contemporary approach to diagnosis and evaluation of renovascular hypertension. Urol Clin North Amer 2001;28(4):781-791.
- van Jaarsveld BC, Krijnen P, Pieterman H. et al The effect of ballon angioplasty on hypertension in atheroclerotic renal-artery stenosis. N Engl J Med. 2002;342:1007-1014.
- Edwards JM Zaccardi M, Strandness DE. A preliminary study of the role of duplex scanning in defining the adequacy of treatment of patients with renal artery fibromuscular dysplasia. Vasc Surg 1992;15:604-609.
- Paulsen D, Klow NE, Lien B, Fauchald P. Treatment of renal artery stenosis. Tidsskr Nor Laegeforen 2001;121(28):3264-3269.
- Greener M. Renovascular hypertension remains raised following surgery. Available at: http://www.cardiosource.com/journal/journal/article?accronym=CARRS%format=abstract&uid=PHS00086636301003662.
- Sukanya M, Gombar KS, Charu D, Das A. Anesthetic management of a patient with Klippel-Feil syndrome. J Anesth 2001;15:53-56.
Review from Roberto Cuan Ravinal, PhD. Departamento de Patologia. Faculdade de Medicina de Ribeirăo Preto. USP-Ribeirăo Preto. Brazil
Review from Hélio Teixeira, MD. PhD. Professor Titular e Livre Docente do Departamento de Clínica Médica. Universidade Federal de Uberlândia. Uberlândia (MG). Brasil
Key words: Klippel-Feil syndrome, renal artery stenosis, and arterial hypertension.
ABSTRACT
We report one patient with Klippel-Feil (KFS) syndrome, other associated anomalies, uncontrolled arterial hypertension, and renal artery stenosis. Because this patient underwent for surgical revascularization with unsuccessful result, all proposed way of treatments are revised, and we have hypothesized that probably for patients with KFS and unilateral renal artery stenosis, medical treatment with ACE inhibitors can provide more benefits than surgical revascularization or percutaneous transluminal angioplasty. We considered that those patients should be manage by a team of medical doctors being aware of their common associated anomalies, identifying all of them when it is possible then, making an integral evaluation of the each individual situation for establishing their medical priorities in order, and then address its treatments accordingly. If at this stage any surgical treatment is required, is important to bring those problems to the anesthesiologist’s attention for a very careful manipulation of the neck and head during induction of anesthesia. The final results will be strongly related with the capacity of management of the underlying cardio-respiratory, renal, skeletal, urogenital, and nervous system problems. . We also propose the term of Klippel-Feil syndrome "Plus" for those patients with cervical vertebral fusion and many other associated deformities rather than to add new eponyms to the long list that already exist.
KEY WORDS
Klippel-Feil syndrome; renovascular hypertension; renal artery stenosis.
INTRODUCTION
We present a young patient with Klippel-Feil syndrome (KFS) plus a wide variety of other deformities, uncontrolled hypertension, and unilateral renal artery stenosis. The management of renal artery stenosis shows some controversial aspects that we will discuss in relation with the management of KFS.
Secondary hypertension due to renovascular diseases remains a leading of potentially correctable hypertension, and new advances in percutaneous trans- luminal angioplasty with stenting and in renovascular surgical techniques have driven interest in afford this problem trough those ways of treatment,1 Surgical revascularization of renovascular disease feasible with a reasonable amount of morbidity and effective in controlling blood and preserving renal function in the majority of cases,2 however in patients with KFS other consideration should be made.
KFS is a congenital malformation due to an abnormal fusion of two o more vertebral bodies at the cervical region, those cervical anomalies are due a failure of normal segmentation of cervical somites during the third and eight weeks of gestation. Most of the patients present with decrease flexion and extension of the neck and almost complete inability to rotate the neck that is short on examination, and a low hairline is always noted. KFS can present with various craniofacial and otolaryngological abnormalities e.g. cleft lip and occasionally skeletal, urogenital or cardiovascular anomalies. Dominant and recessive forms of this heterogeneous syndrome have been classified into four KFS genetic classes;3 combinations of KFS and vertebral artery dissection,4 RAS and aneurysmatic dilatation of internal carotid artery in tuberous sclerosis5 among other combinations have been reported.6 7 8 9
Sometimes neurological problems due to craniocervical junction anomalies like Arnold Chiari malformations type I, platybasia, or basilar invagination can be seen, also genito-urinary problems such as: hydronephrosis, renal ectopia, renal agenesia, horseshoe kidney, double collecting system, and bilateral tubular ectasies. Medical and/or surgical treatments are dependent upon the congenital anomalies present in the syndrome. Undiagnosed hidden anomalies are close related with poor prognosis, in other words: some hidden anomalies can be fatal.10 From our knowledge in our patient there is a novel combination of problems no reported to the medical literature previously.
CASE REPORT
A 15-years-old male patient from Mhlakulo Health Center is referred to Neurology Out Patient Clinic in Umtata General Hospital to complete some clinical investigations. At arrival the patient denied any complaint but is admitted because on the general physical examination some anomalies were observed. The patient was born as the fourth child to healthy non-consanguineous parents. The family history was unremarkable; pregnancy and birth were normal. When he was near the age of 4 years someone noticed "an elevation of the right shoulder" but no growth deficiency in stature is noticed. At admission his weight was 57 kg, his height 160 cm, and his head circumference 57 cm. On the face hypertelorism and mild micrognathia were observed, high narow palate, bilateral microtia, short neck, and low hairline were also noticed. General examination also showed a remarkable chest asymmetry with scoliosis, muscle wasting on the left arm, hand, and wide separation between 3rd and 4th finger (Figure 1)
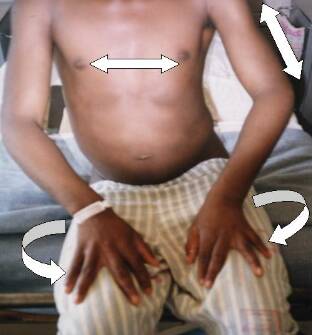
On the lower limbs: mild gigantism of the right big toe, lymphedema of the feet, port-wine stain and "birthmark"(cutaneous capillary malformations) were well defined, the nails and teeth were normal. He was well orientated and no language or speech problems were detected, recent memory and sensory attention were altered, and mild-moderate mental retardation were confirmed, motor system examination showed a decreased muscle power in proximal region predominantly with symmetrical hypotrophy on the left arm, and muscle wasting on the right suprascapular area. Apart from confirmed high blood pressure (174/135 mmHg), cardiac and respiratory systems showed unremarkable findings. Abdomen was prominent and the inferior border of the liver at 4 cm below the right inferior costal margin is palpated.
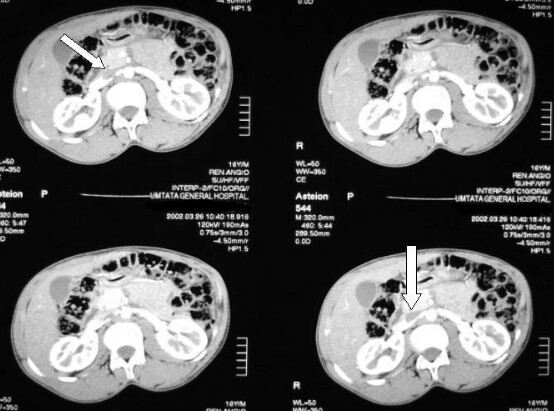
Complementary exams showed: normal full blood count, mild elevation of urea and normal electrolytes, glucose, liver function tests, thyroid function tests, and kidney function tests, within normal limits. Elevated plasma renin activity after captopril administration was confirmed, and radiographic studies showed vertebral fusion between C6-7, moderate scoliosis, Sprengel deformity (congenital supra-elevation of the scapula bone), left omovertebral bone, on X-rays of the craniocervical region, the superior border of the odontoid process of C2 is 6 mm above Chamberlain’s line. CT Scan of the brain showed radiological signs of leucoencephalodystrophy on the cerebral hemispheres. CT angiography showed a right RAS (Figure 2); the patient was transferred to another hospital for surgical treatment of the stenosed artery without remarkable improvement of the arterial hypertension, and he died soon after it.
Ethical considerations
Informed concert was obtained and confidentiality retained.
COMMENTS
Differential diagnosis.
Klippel-Trenaunay syndrome or Klippel-Trenaunay-Weber syndrome (KTWS) is generally accepted, when there are enlargement of the soft tissue, bony hypertrophy, port-wine stain, venous malformations and lymphatic abnormalities; in our patient we could not investigate arterio-venous fistulae by phlebography and arteriography because patient died after the surgical revascularization due to anesthetic and pulmonary complications. KTWS is an uncommon disease (only 310 cases have been published) due to a congenital malformation of the deep venous system with agenesis, hypoplasia or segmental atresia, the etiology is not clear however seems to be related with diffuse mesodermal abnormalities during fetal development and genetic mutations. In 1993, one patient with KTWS an associated renal artery aneurysm was reported.11 We can not demonstrate any relationship between KFS and KTWS if there is any, but we know that KFS can be associated to similar problems or even other ones, reason why we prefer to nominate it as KFS "plus." We personally believe that it is an anecdotic coincidence.
Association of KFS with Sprengel deformity, omovertebral bone and abnormalities on the fingers had been described by Larson12 in members of the same family, these authors considered it as a novel association or syndrome but we considered it is a different clinical manifestation of the same genetic disorder.
Alagille syndrome with associated renovascular hypertension should also be distinguished, the association of at least three of the following five abnormalities characterizes it: chronic cholestasis, peripheral pulmonary stenosis, vertebral arch defects, embryotoxon, and typical facies. Tubulointerstitial nephritis, renal tubular acidosis, and renal artery stenosis have been noted in Alagille syndrome but those typical features of Alagille syndrome have no been documented for our patient.
Kidneys
Abnormalities of the kidneys increase in frequency when there is auricular deformities (microtia), particularly when the patient is afflicted with other manifestations of facial underdevelopment; some patients have hypospadius or vaginal agenesis, and abnormalities of their renal collection systems. However, they can easily live with just one kidney, therefore to see patients with microtia and any life-threatening renal consequences from these system abnormalities is very uncommon, of course living with extremely high diastolic hypertension has a different prognosis.
Renovascular hypertension (RVHT) and RAS.
Opposite situation, like postural hypotension in patient with cervical cord compression (C2-C3) and selective damage of the descending autonomic fibers due to craviocervical anomaly and KFS, has been reported.13
Approximately one-fifth of the South African population suffer of arterial hypertension (HTA); the national prevalence rate of 21% is equivalent to other industrialized countries and greater than many developing countries; nearly half South African population still rural and much of the African urban population now rapidly adopting Western lifestyle habits therefore prevalence rates will increase with time.14
RVHT refers to HTA that is caused by renal hypoperfusion due to a flow-limiting vascular stenosis and is corrected by either surgical or percutaneous revascularization
Its important lies in the fact that it is potentially correctable, thus, it is imperative that patients at highest risk for RVHT be selected from the hypertensive population. RVHT must be distinguished from RAS since one condition frequently exists without the other and the presence of both renovascular disease and HTA does not necessarily implicate causality. In true RVHT, the kidneys takes charge of blood pressure and will do what it takes to push blood pressure high enough to force blood through the blocked artery. This can be diagnosed with functional test that measure glomerular filtration rate before and after blockade of renin-angiotensin system with ACE inhibitors.15To approach that differentiation is recommended to consider that RAS is merely the presence of anatomic stenosis of the renal artery (usually > 70%), whereas true renovascular hypertension is that anatomic diagnosis coupled with renin-dependent hypertension.
Ideally, the hypertension should be ameliorated by correction of the renal artery stenosis. The predictive value of any screening test is a function of the accuracy (sensitivity/specificity) of the test and the prevalence of the disease within the population screened. Sensitivity refers to the probability that a test will be positive when it is applied to a person with a disease. Specifity refers to the probability that a test will be negative when applied to a person free of disease. Provocative captopril tests should be applied only to hypertensive patients thought to have a moderate suspicion of RVHT based on the usual clinical clues.16
Pathophysiology of RAS.
RVHT results when a vascular stenosis leads to renal ischemia and elevation of renin release from the affected kidney, that constriction of the renal artery leads to a cascade of important hemodynamic and humoral events within the affected kidney. If RAS is significant, a reduction in ipsilateral renal artery perfusion pressure occurs that stimulates renin release from the juxtaglomerular apparatus and augments intrarenal angiotensin II production. In the peripheral circulation, angiotensin II promotes systemic vasoconstriction and aldosterone secretion with its attendant sodium retention. The increase in total peripheral resistance and salt retention may contribute to an elevation of mean arterial blood pressure. Within the affected kidneys, the angiotensin II-dependent renal vasoconstriction attenuates the fall in renal blood flow and also affects the glomerular filtration rate by modulating vascular tone of the afferent and efferent renal arterioles. Angiotensin II preferentially increases resistance of the efferent arteriole to maintain transcapillary pressures within the glomerulus that maintain the glomerular filtration rate of the affected kidney.
ACE inhibition interrupts the renin-angiotensin-aldosterone system pathway by preventing the conversion of the decapeptide angiotensin I to the octapeptide angiotensin II such that the vasoconstrictor and aldosterone-stimulating effects of angiotensin II are blocked. ACE inhibition acts as a pharmacological tool to investigate the role of angiotensin II in the pathophysiology of RAS on systemic hemodynamics and assessing a potential plasma renin activity response to ACE inhibition.16
Currently captopril renography seems to be more sensitive and specific screening test than the captopril plasma renin activity test,16 mainly if it is in excess of 90 % or even more but unfortunately that test is not available in our region at the present moment.
Treatment options
The optimal treatment for arterial hypertension due RAS is still a controversial problem. Current treatment options are medical therapy (angiotensin convertin enzyme inhibitors), percutaneous transluminal angioplasty with or without stetting, and surgical reconstruction. Some experts favor surgical revascularisation because of occasional angioplasty failure and the risk of deterioration of renal function after angioplasty.17 Has been clearly established that for those patients who have atherosclerotic RAS with normal or mildly impaired renal function, primary angioplasty was not more effective than antihypertensive drugs alone for reducing blood pressure or limiting disease progression.18
However has been accepted that angioplasty and stenting of stenosed renal arteries normalizes renin secretion by both treated and contralateral kidneys, and improve the function of the treated kidney, but for young patients with non-atherosclerotic RAS the chance for reducing blood pressure by angioplasty is and is not certain; considering that other vascular lesions could be present (Takayasu’s disease) is not, however when there is not coexisting renal parenchyma disease, when there is not progression to renal artery occlusion, no loss of renal mass, and no result in renal failure, those patients respond to angioplasty.19 Paulsen et al performed 591 renal angioplasties in 419 patients with significant renal artery stenosis with better results in patients with fibromuscular dysplasia and concluded: angioplasty can be done in selected patients.19
Because renovascular hypertension remains raised despite surgery, although antihypertensive consumption declines some authors have postulated that uncorrected media/lumen ratio in resistance arteries does not cause hypertension,20 Prevalence of secondary hypertension remains unknown and severe hypertension due to RAS and an associated KFS had not been before-cited; to the best of our knowledge this is the first report on this type of association in the medical literature.
Surgical reconstruction of the stenosed renal artery take time under anesthesia and the patient’s body is forcibly moved in turning maneuvers including the head and neck for inducing anesthesia therefore risk of provoke complications increase with, mainly in those patients who the 100 % of underlying problems had not been previously identified. It is important to realize that if the congenital anomalies are picked up at an early stage, the damage is less harsh during intervention. Although the following situation has not been reported yet if any patient with bilateral renal artery stenosis (ACE inhibitors are contraindicated) undergo for surgery then anesthetic consideration should be disscused.21 for patients with KFS and unilateral renal artery stenosis the treatment of choice should be medical with ACE inhibitors because the high risk of anesthetic complication for patients with KFS among other reasons before mentioned. We also propose the term of Klippel-Feil syndrome "plus" for those patients with cervical vertebral fusion and other associated deformities rather than to add another eponym to the long list that already exist.
Acknowledgments
The authors wish to acknowledge Mrs. Lourdes Margarita Guillermina Valdes Perez for her contributions.
REFERENCES
Comment Reviewer
Prof. Roberto Cuan Ravinal. Departamento de Patologia. Faculdade de Medicina de Ribeirăo Preto. USP-Ribeirăo Preto. Brazil
Patients with Klippel-Feil Syndrome may be at increased of risk of significant genitourinary tract anomalies as ectopic kidney and renal agenesis, and have increase chance of developing nephrolitiasis.
In this paper the authors describe one patient with Klippel-Feil Syndrome, renal artery stenosis, uncontrolled arterial hypertension and other associated anomalies.
Anomalias arteriais, como estenose de artéria subclávia1, aneurisma de artéria renal2 e coarctaçăo de aorta3, săo descritas em pacientes portadores de síndrome de Klippel Feil, ao lado de outras malformaçőes congęnitas.
REFERENCES:
Comment Reviewer Prof. Hélio Teixeira. Professor Titular e Livre Docente do Departamento de Clínica Médica. Universidade Federal de Uberlândia. Uberlândia (MG). Brasil
O presente artigo relata o primeiro caso de estenose de artéria renal com hipertensăo renovascular associado ŕ síndrome de Klippel Feil. O paciente foi a óbito após cirurgia para correçăo da estenose renovascular.
A lesăo da coluna cervical - característica desta síndrome - pode dificultar o procedimento da anestesia geral4, além de favorecer o surgimento de seqüelas neurológicas definitivas secundárias a pequenos traumas em nível cervical5 nesses pacientes.
1. Indian J Pediatr 2002 May;69(5):441-2
2. Br J Urol 1993 May;71(5):617-8
3. Cardiovascular Pathol 2003 Mar-Apr;12(2):115-7
4. Anesth Analg 2001 Feb;92(2):514-6
5. BMC Fam Pract 2002 Apr11;3(1):6