Indice del volumen Volume index
Comité Editorial Editorial Board
Comité Científico Scientific Committee
- Epilepsy under treatment with carbamazepine (600 mg/day)
- Hypertension treated with enalapril (10 mg/day) plus atenolol (25 mg/day)
- Pulmonary thromboembolism treated with warfarin (10 mg/day)
OXCARBAZEPINE INDUCED HYPONATREMIA:
A POTENTIAL EXPLANATION OF ITS PHYSIOPATHOLOGY.
Carlos G. Musso1-3, Vilas M1-3, Aparicio C1, Bevione P1,
Reynaldi J1, Rojas J2, Jauregui R3, Algranati L1.
1Nephrology and 2 Neurology Departments.
3 Centro Médico Agustin Rocca
Hospital Italiano de Buenos Aires.
Buenos Aires. Argentina
carlos.musso @ hospitalitaliano.org.ar
Rev Electron Biomed / Electron J Biomed 2009;1:32-35
SUMMARY
Carbamazepine and oxcarbazepine are antiepileptic drugs which can induce hyponatremia, being this disorder more frequent with the latter.
In this report we present a clinical case regarding an oxcarbazepine induced hyponatremia, and we hypothesized that oxcarbazepine could induce hyponatremia as a consequence of its influence on distal nephron where it could promote free water retention, urinary sodium loss, or both of them.
Besides, we proposed that a greater tubular sesitivity to oxcarbazepine than to carbamazepine could explain the different hyponatremia inducing capability between these two drugs
KEY WORDS: Oxcarbazepine. Hyponatremia. Physiopathology
RESUMEN
La carbamazepina y la oxcarbazepina son drogas antiepilépticas potencialmente inductoras de hiponatremia, siendo este disturbio más frecuente con ésta última.
En este reporte presentamos un caso de hiponatremia inducida por oxcarbazepina, y proponemos una potencial explicación fisiopatológica para esta entidad, a la cual se la considera consecuencia de un aumento a nivel de los túmulos colectores de la reabsorción de agua libre, de la pérdida urinaria de sodio, o de ambos fenómenos combinados.
Además, postulamos que la mayor propensión a la aparición de hiponatremia con el uso de oxcarbazepina respecto del empleo de carbamazepina podría ser consecuencia de una mayor sensibilidad de los túmulos colectores a la primera de las drogas mencionadas.
PALABRAS CLAVE: Oxicarbazepina. Hiponatremia. Fisiopatología
INTRODUCTION
Hyponatremia is one of the most frequent electrolyte disorders associated to medication, being those drugs prescribed for psychological or neurological disorders the most dangerous ones in this sense1.
Carbamazepine and oxcarbazepine are antiepileptic drugs which can induce hyponatremia, an adverse effect usually asymptomatic in the setting of these dugs2,3.
Even though, both drugs are chemically related, since oxcarbazepine is a ketoderivative of carbamazepine, hyponatremia seems to be more associated to oxcarbazepine3-5. There is no explicative hypothesis for such difference in the literature6, then we present a case of oxcarbazepine induced hyponatremia, and potential explanation for its physiopathology in the present clinical report.
CASE REPORT:
Female patient, 71 years old, who had the following antecedents:
Since it was difficult to reach an adequate anticoagulation status in this patient, it was interpreted that the inductor enzimatic effect of carbamazepine could explain this refractory to anticoagulation. Then, it was decided to change the antiepileptic drug from carbamazepine (600 mg/day) to oxcarbazepine (600 mg/day) which has a lesser enzimatic induction effect.
Fourty eight hours after this change, the patient developed an asymptomatic hypotonic hyponatremia, with normal extracellular fluid, lowering her serum sodium level from 138 mmol/l progressively to 120 mmol/l.
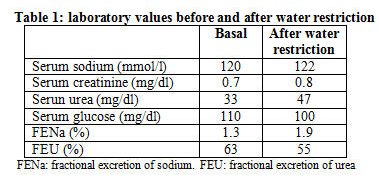
Since, it was intended to keep the oxacarbazepine treatment, water restriction was effectively implemented (documented by a reduced fractional excretion of urea), but there was no amelioration in her serum sodium level (Table 1).
Then, enalapril, another potetial cause of hyponatremia, was discontinued and hypertension was controlled increasing her previous atenolol dose (25 mg/day to 50 mg/day). However, despite the above described therapeutical changes, her hyponatremia was not solved.
Finally, oxacarbazepine was stopped and carbamazepine was reintroduced as her antiepileptic treatment, while anticoagulation was handled using subcutaneous low weight heparin. Fourty eight hours after these changes serum sodium levels went back to normal range.
DISCUSSION:
Although structurally related to carbamazepine, oxcarbazepine has several clinically relevant advantages over the former, including a more favorable pharmacokinetic profile and a better tolerability.
Because the metabolism of oxcarbazepine follows non-oxidative pathways, it has a lower propensity to induce hepatic oxidative enzymes and a reduced potential for drug-drug interactions. Additionally, oxcarbazepine does not undergo autoinduction3,7.
Even though, early reports suggested that carbamazepine could induce excessive release of vasopressin and lead to inappropriate secretion of antidiuretic hormone, more recent studies have not found such hormonal increase8.
It was documented in another study that after a water load, serum sodium and free water clearance were diminished in persons (patients or volunteers) who were on oxcarbazepine. Besides, oxcarbazepine induced hyponatremia was not associated with significant elevation in serum vasopressin levels. These findings indicate that oxcarbazepine-induced hyponatremia is not attributable to the syndrome of inappropiate secretion of antidiuretic hormone7-8.
Moreover, it was also reported that serum natriuretic peptides levels were decreased in these hyponatremic patients7. Actually, in a study performed in patients on oxcarbazepine, serum aldosterone levels were increased in six normonatremic patients while these hormonal levels remained stable in 4 patients who were suffering from hyponatremia, suggesting that an increase in aldosterone levels could involved a compensatory mechanism to prevent hyponatremia in these patients3.
Besides, it is already known from Edelman equation (natremia = free water / sodium + potassium) that hypotonic hyponatremia can be basically a consequence of an increase in free water body content, sodium deplection or a combination of both mechanisms9.
Then, based on the above provided information, it could be hypothesized that the modification of collecting tubules induced by oxcarbazepine could lead them to an increased water reabsorption or/and sodium loss. Besides, a greater induction of these tubular changes in patients on oxcarbazepine respect to the cabamazepine induced ones, could explain the reported higher incidence of hyponatremia in patients on oxcarbazepine.
CONCLUSION:
Oxcarbazepine could induce hyponatremia as a consequence of its influence on distal nephron where it could promote free water retention, urinary sodium loss, or both of them.
A greater tubular sesitivity to oxcarbazepine influence respect to carbamazepine one could explain the different hyponatremia inducing capability between these two drugs.
REFERENCES
- 1) Cía P, Quero J, Rodrigo MD, Bondía A, Acin P, Aisa O. Hiponatremia sintomática a tratamientos con oxcarbacepina. Revista de la sociedad española del dolor. 2006; 13: 395-398
2.- Pendlebury SC, Moses DK, Eadie MJ. Hyponatraemia during oxcarbazepine therapy. Hum Toxicol. 1989 ; 8: 337- 44
3.- Isojärvi J, Huuskonen U, Pakarinen AJ, Vuolteenaho O, Myllylä V. The regulation of serum sodium after replacing carbamazepine with oxcarbazepine. Epilepsia. 2001; 42: 741-745
4.- Holtmann M, Krause M, Opp J, Tokarzewski M, Korn-Merker E, Boenigk HE. Oxcarbazepine-induced hyponatremia and the regulation of serum sodium after replacing carbamazepine with oxcarbazepine in children. Neuropediatrics. 2002;33:298-300
5.- Dong X, Leppik IE, White J, Rarick J. Hyponatremia from oxcarbazepine and carbamazepine. Neurology.2005; 27;65:1976-1978.
6.- Van Amelsvoort T, Bakshi R, Devaux CB, Schwabe S. Hyponatremia associated with carbamazepine and oxcarbazepine therapy: a review. Epilepsia. 1994;35:181-188
7.- Oxcarbazepine: drug information. Lexi-Comp. 2008
8.- Sachdeo R, Wasserstein A, Mesenbrink J, D´Souza J. Effects of oxcarbazepine on sodium concentration and water handling. Ann Neurol. 2002; 51: 613-620
9.- Adrogue H, Wesson D. Salt & Water. Houston. Libra & Gemini. 1993
Received: March 9, 2009.
Published April 2, 2009.