Indice del volumen Volume index
Comité Editorial Editorial Board
Comité Científico Scientific Committee
- Suitable randomization
- blinding of the assignment
- Blinding of the Intervention
- Complete follow up
- Blinding of the results measurement
VALUE OF STRONTIUM IN THE PREVENTION OF BONE FRACTURES CAUSED BY FALLS IN VERY OLD PATIENTS WHO SUFFER FROM PRIMARY OSTEOPOROSIS:
A SYSTEMATIC REVISION
Carlos G. Musso, Ricardo Jáuregui, Agustín Ciapponi
Centro Médico Agustin Rocca. Hospital Italiano de Buenos Aires.
Buenos Aires. Argentina
carlos.musso @ hospitalitaliano.org.ar
Rev Electron Biomed / Electron J Biomed 2011;1:68-76.
Comment of the reviewer Dr. Hugo Alberto Schifis. Presidente de la Sociedad Argentina de Gerontología y Geriatría. Facultad de Ciencias Médicas de la Universidad de Buenos Aires. Argentina..
Comment of the reviewer Dr. Ignacio Martínez Sancho MD. Médico de Familia. Centro de Salud "Gamonal Antigüa". Burgos, España.
SUMMARY:
Introduction: Since between 25-30% bone fractures, and 60% hip fractures in the general population are common in the subgroup which correspond to very old women. This happens due to the high predominance of primary osteoporosis and the incidence of falls which are characteristic of such group; thus, we have decided to investigate, through a systematic revision of the bibliography, the value of strontium in the prevention of bone fractures caused by falls in very old patients who suffer from primary osteoporosis.
Material and Method: A systematic revision of the literature was carried out following the recommendations of the Cochrane methodology. Out of the 8 documents initially recovered, only two were included (2 independent reviewers selected, evaluated and extracted the data from the included tests) since such tests were the only ones which complied with the eligibility criteria to be tests performed on a population of very old patients: older than 74 years old, thus reaching a total amount of 2616 patients who took part in this test.
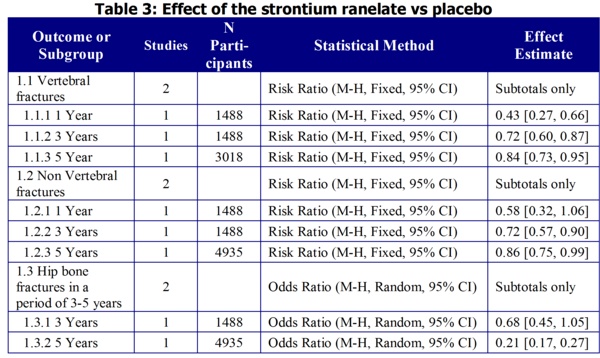
Results: Despite the abundance of information in favour of the treatment using strontium, there is a relative risk in the case of non-vertebral fractures one year after treatment which goes through unit: 0.58 [0.32, 1.06]. Regarding the risk of fracture at the hip level, there are certain differences when it is compared with the aforementioned data. On the one hand, the reduction of the risk of fractures (32%) after 3 years of treatment with strontium ranelate documented by the Seeman test 2006 did not reach statistical significance (p=0.112), and its relative risk goes through unit: 0.68 [0.45, 1.05]
Nevertheless, the Reginster 2008 test showed that after 5 years of treatment with strontium ranelate there was a bigger reduction (43%) which was statistically significant (p=0.036) (Tables 1 and 4).
Such data could mean that the hip bone may need a longer period of exposure to strontium to benefit from an effective reduction of its risk of fracture.
Conclusions: The biggest reduction in the risk of fracture was evidenced in vertebral fractures compared with the non vertebral fractures, even when the IC 95% overlap significantly. Additionally, the biggest anti-fracture effect was documented one year after treatment using strontium ranelate in comparison with the 3 years of the same treatment, as well as a bigger reduction in the risk of fracture after 3 years compared with five years of it. We conclude that there are tests that support the use of strontium ranelate, in 2 grams doses administered daily for at least 3 years, to achieve a significant reduction of the incidence of vertebral as well as non vertebral fractures in very old women with primary osteoporosis.
KEY WORDS: Strontium. Fractures. Osteoporosis.
RESUMEN: VALOR DEL ESTRONCIO EN LA PREVENCIÓN DE FRACTURAS ÓSEAS SECUNDARIAS A CAÍDAS EN PERSONAS MUY ANCIANAS PORTADORAS DE OSTEOPOROSIS PRIMARIA: UNA REVISIÓN SISTEMÁTICA
Introducción: dado que entre el 25-30% de las fracturas óseas, y 60% de las fracturas de cadera de la población general, acontecen en el subgrupo correspondiente a las mujeres muy ancianas. Esto se debe a la alta prevalencia de osteoporosis primaria e incidencia de caídas característica de este grupo, hemos decidido investigar el valor del estroncio en la prevención de fracturas óseas secundarias a caídas en personas muy ancianas portadoras de osteoporosis primaria por medio de una revisión sistemática de la bibliografía.
Material y Métodos: se realizó una revisión sistemática de la literatura siguiendo las recomendaciones de la metodología Cochrane. De los 8 los documentos inicialmente recuperados, sólo 2 terminaron siendo incluidos (2 revisores independientes, seleccionaron evaluaron y extractaron los datos de los estudios incluidos) por ser los únicos que cumplían con el criterio de elegibilidad de ser estudios realizados sobre una población de pacientes muy ancianos: mayor de 74 años de edad, totalizando 2616 personas en estudio.
Resultados: a pesar la abundancia de datos a favor del tratamiento con estroncio, hay un riesgo relativo para fractura no vertebral al año de tratamiento que pasa por la unidad: 0.58 [0.32, 1.06]. En cuanto al riesgo de fractura a nivel de la cadera, existe ciertas diferencias respecto de los datos antes mencionados. Por un lado, la reducción del riesgo de fractura (32%) luego de 3 años de tratamiento con ranelato de estroncio documentada por el estudio Seeman 2006 no alcanzó significación estadística (p=0.112), y su riesgo relativo pasa por la unidad: 0.68 [0.45, 1.05]
Sin embargo, el estudio Reginster 2008 demostró luego de 5 años de tratamiento con ranelato de estroncio una reducción mayor (43%) y estadísticamente significativa (p=0.036).
Estos datos podrían significar que tal vez el hueso de la cadera requiera un tiempo de exposición más prolongado al estroncio para verse beneficiado en una efectiva reducción de su riesgo de fractura.
Conclusiones: la mayor reducción del riesgo de fractura se vio en fracturas vertebrales respecto de las no vertebrales, si bien los IC 95% se superponen ampliamente. Así mismo, el mayor efecto anti-fractura se documento luego del año de tratamiento con ranelato de estroncio respecto de los 3 años del mismo, así como también se documento una mayor reducción del riesgo de fractura a los 3 años de tratamiento respecto de los 5 años del mismo. Concluimos que hay pruebas que apoyan la utilidad del ranelato de estroncio, en dosis de 2 gramos diarios suministrado durante al menos 3 años, para reducir significativamente la incidencia de fracturas vertebrales y no vertebrales en mujeres muy ancianas con osteoporosis primaria.
PALABRAS CLAVE: Estroncio. Fracturas. Osteoporosis.
INTRODUCTION
Approximately, between 25-30% bone fractures, and 60% hip fractures of the general population occur in the very old women subgroup (older than 75 years old). This is due to the high prevalence of primary osteoporosis and the incidence of falls which is characteristic of this group 1.
Osteoporosis is a skeletal disorder which is characterized by the low bone mass and the deterioration of the micro architecture of the bone which causes the increase of bone brittleness and the risk of fracture 2,3 while falls as a geriatric syndrome are a complication characteristic of the walking disorder typical in the old.
Taking into consideration the above mentioned information and the fact that this age group is obviously increasing in the western world, the prevention of this pathology (osteoporosis) and its complications (bone fractures, immobility, etc) have a clear economic impact on the budgets of health insurance systems 4.
Bone brittleness, which characterizes osteoporosis results from an imbalance in bone remodelling: bone resorption exceeds bone formation, and the augment in the remodelling rate at the tissue level5. In 1994, a team from the World Health Organization proposed that an individual with bone density higher than 2,5 standard deviations (SD) under the average of a young adult suffers from osteoporosis6
The pharmacological treatment to prevent and treat this entity includes two kinds of main drugs: anti resorption agents and anabolics. The anti resoption agents increase bone resistance since they lower osteolytic action. On the contrary, the anabolic agents increase bone resistance since they augment bone mass due to an increase in osteoblastic activity7,8.
However, there is a new oral agent, strontium ranelate, which has the particular benefit of not only being an inhibitor of bone resorption (osteoclastic activity), but also of stimulating the formation of such tissue (osteoblastic activity). From the chemicals point of view, this product consists of two atoms of the divalent cation of stable strontium (natural element) and an organic fraction (ranelic acid) which dissociates at a gastrointestinal level. Strontium is a cation and is closely related, from the physical point of view, with calcium, an active component of the skeleton. The ranelic acid is an organic molecule, extremely polar without pharmacological activity. Although several doses of strontium ranelate have been tried (0.125 - 2 g), the most recommended doses proved to be 2 grams a day 9,10.
In light of the above mentioned information we decided to investigate the value of strontium ranelate in the prevention of bone fractures caused by falls in very old patients who suffer from primary osteoporosis through a systematic revision of the bibliography.
MATERIAL AND METHOD:
A Systematic Revision was carried out, for which initially we proceeded to formulate the following recommended questions as a guide to perform the systematic revision of double blind controlled random essays, which complied with the following selection criteria:
-
1) Patient/problem: very old patients (older than 75 years old) who suffer from osteoporosis (mineral bone density of the lumbar spine of < -2,5 DE). (oldest old/ very old - osteoporosis)
2) Intervention: therapy using 2 grams/day of strontium at least for 2 years (besides also receiving calcium 500-1000 mg/day and vitamin D 400-800 UI/day).
3) Comparison: patients who were not treated with strontium: placebo (placebo) but received calcium 500-1000 mg/day and vitamin D 400-800 UI/day
4) Results (main point of interest): bone fracture (radiologically documented) secondary to falls due to senile walking disorder (bone fracture - falls)
Extensive bibliographical research was carried out using key words: the above mentioned ítems (in spanish and in english) and using the strategy recommended by Haynes to look for "links"
1) The information systems or the new systematic books,
2) secondary information sources or good clinical practice guidelines.
UpToDate®
TRIPDATABASE
Guidelines
CMA INFOBASE Clinical Practice Guideline
Evidence in Ambulatory Practice
Scottish Intercollegiate Guidelines Network
3) Systematic Reviews and meta-analysis
4) Complete and extensive research of articles in databases Medline, Embase, Lilacs, following the aforementioned criteria.
5) Additionally, the lists of reference of the included tests were explored and experts on the matter were also consulted.
The period covered by the search was 10 years, in Spanish and English.
Two reviewers independently selected, extracted and evaluated the quality of the tests. A simple method was used to assess such quality:
Selected Tests:
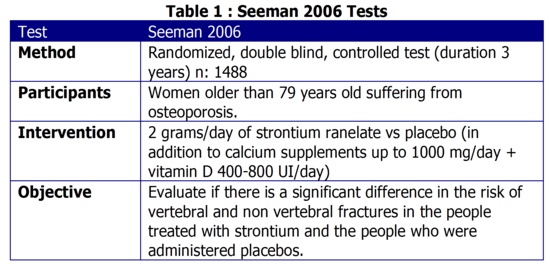
1) Seeman 2006: It is a work which analyses two international tests, which assessed the effect of strontium ranelate (2 g/day) on primary osteoporosis. Such tests were phase III, randomized, double blind, and controlled: Spinal osteoporosis therapeutic intervention (SOTI) and Treatment of peripheral osteoporosis (TROPOS) with a follow up period of 3 years11-13.
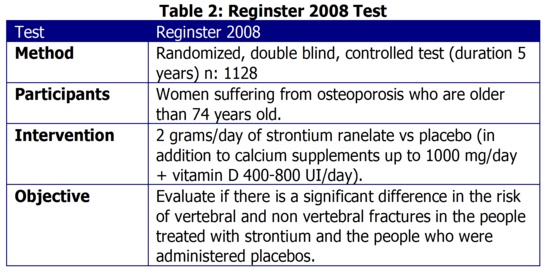
2) Reginster 2008: It is a randomized, double blind, controlled test which evaluated the effect of strontium ranelate (2 gramos/day) on primary osteoporosis with a follow up period of 5 years (continued from the TROPOS test) 14.
Since both tests share patients and both include patients from the TROPOS test, no statistical treatment was carried out (meta-analysis) to the present systematical review.
RESULTS
Number of studied patients:
One of the Studies included 1488 patients ( 151 from SOTI and 1405 from TROPOS) who were all women of 80 years old or older (out of 6740 total patients) (Seeman 2006); the other test included 1128 women older than 74 years old (out of 5091 post-menopausical women), 2616 patients in total.
Duration of the treatment:
3 years (Seeman, 2006)11
5 years (Reginster 2008)14
Dropout rate:
701 patients stopped the test (47.1%) (Seeman, 2006)11
The dropout rate in 5 years was 47% (Reginster 2008)14
Statistical Analysis:
The survival rate analysis was carried out using the Kaplan-Meier survival curves.
The treatment groups were compared using a Cox model (Seeman 2006)11
The treatment groups were compared using a Cox model, and reconfirming using the log rank test (5% type I error)
Analysis of covariance: Student test and the number of patients who showed weight loss: chi square (Reginster 2008)14.
Bone Fractures
When 2 grams/day of strontium ranelate were used, the risk of bone fracture was reduced a 37% a year later (p=0.012) and 3 years after use it was reduced a 22% (p=0.040) (Seeman 2006)11, while in another test the risk of fracture was reduced a 15%: relative risk 0.85 (0.73-0.99) p=0.025 after 5 years of treatment (Reginster 2008)14 (Table 1)
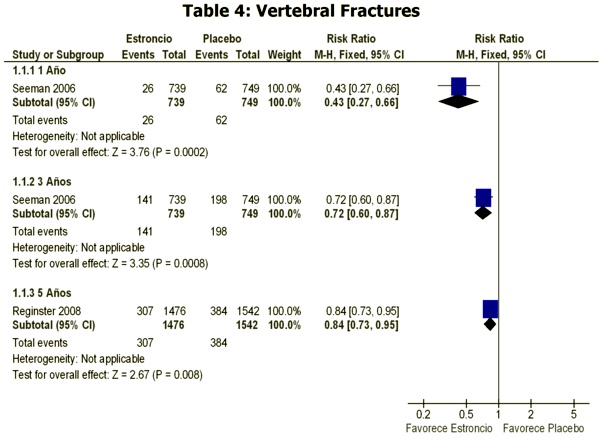
Vertebral Bone Fractures:
The risk of vertebral bone fracture was reduced a 59% (p=0.002) a year later, and a 32% 3 years after use (p<0.013) (Seeman, 2006)11,while such risk was reduced a 24%: relative risk 0.76 (0.65-0.88) p<0.001 after 5 years of treatment (Reginster 2008)14 (Tables 1 and 2)
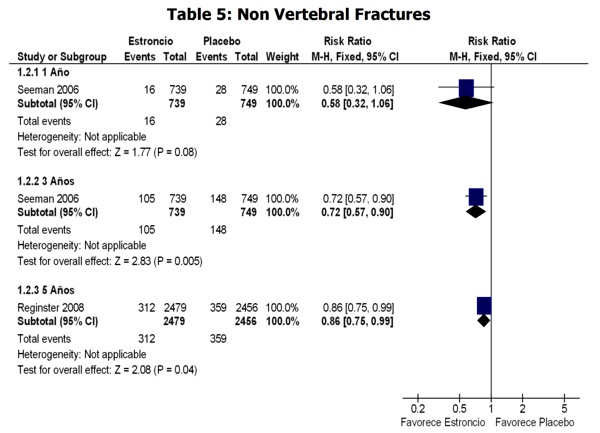
Non Vertebral Bone Fractures:
The risk of non vertebral bone fractures was reduced a 41% a year later (p=0.027), and a 31% 3 years after treatment (p<0.011), while non vertebral large bone fractures (hip, wrist, pelvis, sacrum, clavicule, sternum and humerus) presented a reduction of the 37% (p=0.003) (Seeman, 2006)11 (Tables 1 and 3)
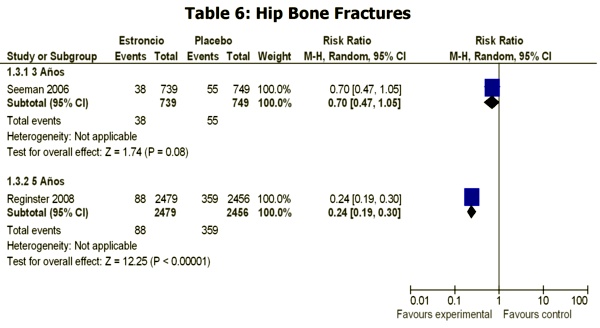
Hip Bone Fracture:
The risk of hip bone fracture was reduced a 32%, without reaching statistical significance (p=0.112) after 3 years of treatment with strontium ranelate (2 gr/day) (Seeman 2006)11, while the risk of hip bone fracture was reduced a 43%: relative risk o 0.57 (0.33-0.97) p=0.036 after 5 years of such treatment (Reginster 2008)14. (Tables 1 and 4)
Adverse Effects
Strontium ranelate was well tolerated; the only adverse effect reported in the group treated was a higher incidence of nausea, diarrhea, headaches, high blood pressure (Seeman, 2006)11, likewise, this drug also proved to be safe in another test, only presenting a higher incidence of nausea, diarrhea, headaches, dermatitis and eczema in the group treated with this drug. The incidence of thromboembolism was not significantly higher in the treated group (Reginster 2008)14.
DISCUSSION:
Two essays complied with the eligibility criteria: such essays researched the effects of strontium ranelate, in doses of 2 grams/day, compared with the placebo in a population older than 74 years old (very old).
Taking the results into consideration, there seems to be a tendency to a higher effect of the treatment a year after its administration (always considering that the confidence intervals (CI) overlapped. The highest reduction in the risk of bone fracture was detected in vertebral compared with non-vertebral fractures (Tables 3, 4 and 5). In addition, the highest anti-fracture effect was documented a year after treatment with strontium ranelate in comparison with the 3 year treatment, a higher reduction was also documented in the risk of bone fracture after 3 years of treatment comparing it with the 5 years of the same treatment (Tables 3, 4 and 5). The first phenomenon (higher reduction in the risk of bone fracture at the vertebral level) could be due to a higher effect of the strontium ranelate on the vertebral bone mineral density versus non-vertebral. Regarding the second phenomena (higher reduction of the risk one year after treatment compared with the 5 year treatment), could be explained due to the fact that the bone tissue is strengthened when it is exposed to the effect of strontium for a longer period of time.
Despite the amount of data supporting the treatment with strontium, there is a relative risk in the case of non vertebral bone fracture after one year of treatment through the unit: 0.58 [0.32, 1.06].
Regarding the risk of bone fracture at the hip level, there are certain differences with the above mentioned data. On the one hand, the reduction of the risk of bone fracture (32%) after 3 years of treatment using strontium ranelate documented in the Seeman 200611 test was not statistically significant (p=0.112). The relative risk even through the unit: 0.68 [0.45, 1.05]
However, the Reginster 200814 test demonstrated that after 5 years of treatment with strontium ranelate there was a higher reduction (43%) which was statistically significant (p=0.036) (Tables 3 and 6).
These data could indicate that the hip bone may require a longer time of exposure to strontium to benefit from an effective reduction in its risk of fracture. A statistical treatment (meta-analysis) could not be carried out on this systematic review since the articles on which it is based share patients.
CONCLUSSION:
There are some tests which support the use of strontium ranelate, in 2 gram daily doses administered for at least 3 years, to significantly reduce the incidence of vertebral and non-vertebral fractures in very old women with primary osteoporosis.
REFERENCIAS:
-
1.- Boonen S, Mc Clung M, Eastell R, Fuleihan G, Barton I, Delmas P. Safety and efficacy of risedronate in reducing fracture risk in osteoporotic women aged 80 and older: implications for the use of antiresorptive agents in the old and oldest old. JAGS. 2004; 52: 1832-1839
2.- Consensus Development Conference: Diagnosis, Prophylaxis, and Treatment of Osteoporosis. In: American journal of medicine. Vol. Vol. 94, issue 3. 1993:561.
3.- NIH consensus development panel on osteoporosis prevention and diagnosis. Osteoporosis prevention, diagnosis, prophylaxis and treatment. Journal of american medical association 2001;285:785-95.
4.- Kiel D, Rosen C, Dempster D. Age-related bone loss. American society for bone and mineral research. 2008: 98-102
5.- Seeman E. Pathogenesis of bone fragility in women and men. Lancet 2002;359(9320):1841-50.
6.- WHO Study Group. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO study group. World Health Organization technical report 1994; Vol. 843:1-129.
7.- Riggs BL, Parfitt AM. Drugs used to treat osteoporosis: The critical need for a uniform nomenclature based on their action on bone remodeling. Journal of bone and mineral research 2005;20(2):177-84.
8.- Sorbera LA, CastanËer J, Leeson PA, Bayes M. Strontium ranelate: Treatment and prevention of osteoporosis bone resorption inhibitor bone formation stimulant. Drugs of the future 2003;28(4):328-35.
9.- EMEA. PROTELOS. The committee for medicinal products for human use 2004.
10.- Ammann P, Shen V, Robin B, Mauras Y, Bonjour J, Rizzoli R. Strontium ranelate improves bone resistance by increasing bone mass and improving architecture in intact female rats. Journal of bone and mineral research. 2004; 19(12): 2012-2020
11.- Seeman E, Vellas B, Benhamou C, et. Strontium ranelate reduces the risk of vertebral and nonvertebral fracture in womwn eighty years of age and older. Journal of bone and mineral research. 2006.21; 7: 1113-1120
12.- Reginster J, Seeman E, De Verejoul M, Adami S, Compston J, Phenekos C, Devogelaer J, Diaz Curiel M, Sawicki A, Goemaere S, Sorensen O, Felsenberg D, Meunier P. Strontium ranelate reduces the risk of nonvertebral fractures in postmenopausal women with osteoporosis: treatment of peirpheral osteoporosis (TROPOS) study. The journal of clinical endocrinology & metabolism. 2005; 90(5): 2816-2822
13.- Meunier P, Roux C, Seeman E, Ortolani S, Badurski J, Spector T, Cannata J, Balogh A, Lemmel E, Pors-Nielsen S, Rizzoli R, Genant H, Reginster J. The New England Journal of Medicine. 2004; 350(5): 459-468
14.- Reginster J, Felsenberg D, Boonen S, et al. Effects of long-term strontium ranelate treatment on the risk of nonvertebral and vertebral fractures in postmenopausal osteoporosis. Arthritis & Rheumatism. 2008.58 (6):1687-1695.