Indice del volumen Volume index
Comité Editorial Editorial Board
Comité Científico Scientific Committee
Letters to the Editor / Cartas al Editor
NEUROTRAUMA AND QUATERNARY PREVENTION: NON-USE OF UNNECESSARY MEDICAL INTERVENTION IN NEUROTRAUMATOLOGY AND NEUROCRITICAL CARE
Tariq Janjua MD1, Amit Agrawal MD2,
Luis Rafael Moscote-Salazar MD3
1Department of Critical Care Medicine, Physician Regional Medical Center, Naples, USA.
2 Department of Neurosurgery, All India Institute of Medical Sciences, Saket Nagar, Bhopal 462020, Madhya Pradesh, India.
3Research Department, Colombian Clinical Research Group in Neurocritical Care, Bogota, Colombia.
Email: rafaelmoscote21@gmail.com
Rev Electron Biomed / Electron J Biomed 2022;2:34-36.
Dear editor:
To define and characterize the interventions that can cause risk to the patient and pave the way for procedures, the concept of Quaternary Prevention (Also called P4) is important. In 1986, Doctor Marc Jamoulle (Belgium) proposed the term quaternary prevention1, which has spread worldwide thanks to the work of the Wonca International Classification Committee (WICC)2.
Ethically endorsed, the concept of quaternary prevention emerged as we deal with complex technological and interventional approaches for our patients. Primum non nocere is a Latin expression that frames the concept that any intervention that may cause harm is better than not doing something. Quaternary prevention is linked to this principle that leads us to use any diagnostic, therapeutic, and preventive action that does not lead to any benefit in the outcome3,4.
By applying this approach in the practice of medicine, overmedication reduction and reduction of unnecessary monitoring in patients in the intensive care can be achieved. Rational use of medical quaternary prevention should be imperative in patients with traumatic brain injury in the intensive care. Here we summarize the approach and what are the limitations of this approach in modern clinical practice.
Among the actions that can be an example of quaternary prevention include avoiding hypertonic saline infusion without clear cut cerebral edema, avoiding the use of osmotic therapy without any clear traumatic brain injury or cerebral edema, not getting serial brain imaging with no neurological change, and not doing decompressive hemicraniectomy for irreversible brain injury particular brain stem injury. This list can be exhaustive and neurointensivists, neurosurgeons, intensivists, nursing staff, and other ancillary staff need to be aware and think through the process of offering or conducting these actions.
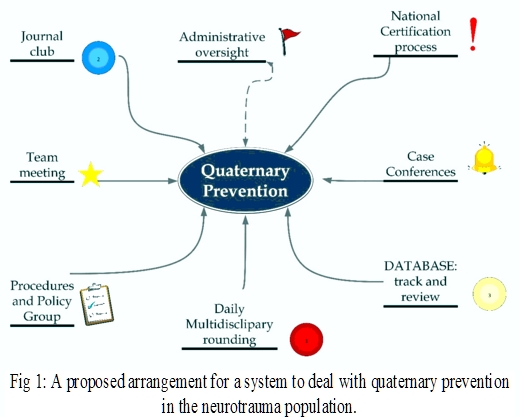
The process to increase quaternary prevention requires regular meetings, case conferences, pathways development, regular review of literature like journal clubs, multidisciplinary rounds, and sometimes root cause analysis (Figure 1).
Once the concept is obvious, the center of excellence for a traumatic brain injury can adopt any pathway which is suitable to that particular system to conduct regular analysis of quaternary prevention. These exercises help to narrow down what is on the stack and what changes are required.
We believe that the incorporation of this concept for the management of neurocritical patients and especially patients with neurotrauma is important. A search for procedures and therapeutic strategies in an adequate balance with what may cause some type of injury to patients must be considered. In current times where the rational use of resources becomes an imperative need, quaternary prevention must be recognized as a scenario that will tend to mitigate deleterious circumstances and that at the same time cost-effective.
REFERENCES
1.-Jamoulle M. Quaternary prevention, an answer of family doctors to overmedicalization. Int J Health Policy Manag. 2015;4(2):61-64.
2. Jamoulle M. Quaternary prevention: first, do not harm. Rev Bras Med Fam Comunidade. 2015;10(35):1-3.
3. Martins C, Godycki-Cwirko M, Heleno B, Brodersen J. Quaternary prevention: reviewing the concept. Eur J Gen Pract. 2018(1):106-111.
4. Gérvas J. Quaternary prevention in the elderly. Rev Esp Geriatr Gerontol. 2012;47:266-269.
CORRESPONDENCE:
Luis Rafael Moscote, MD
Colombian Clinical Research Group in Neurocritical Care,
Bogota, Colombia
Email: rafaelmoscote21@gmail.com
Received: 11/09/2022
Published: 13/09/2022